Emerging NeurotherapeuticTechnologies¶
Chapter 500 | Harrison's 22e · Parts 19-20 – Consultative & Emerging Topics
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- See source text for full details
📑 Table of Contents¶
📋 Figures in This Chapter¶
RAW CONTENT¶
[PAGE 3963] Emerging Neurotherapeutic Technologies 3963 CHAPTER 500 ■ FURTHER READING emerging diagnostic and therapeutic approaches that have the poten- Barabasi A-L et al: Network medicine: A network-based approach to tial to transform the lives of patients with neurologic disorders. These human disease. Nat Rev Genet 12:56, 2011. include technologies to harness plasticity, neuroimaging, neurostimu- Cheng F et al: Network-based approach to prediction and population- lation, and brain–machine interfaces. based validation of in silico drug repurposing. Nat Commun 9:2691, 2018. NONINVASIVE TECHNOLOGIES TO Liu X et al: Robustness and lethality in multilayer biological networks. HARNESS PLASTICITY Nat Commun 11:6043, 2020. Neurologic rehabilitation aims to harness activity-dependent plasticity Loscalzo J et al (eds): Network Medicine: Complex Systems in Human mechanisms to maximize functional restoration. This principle can Disease and Therapeutics. Cambridge, MA, Harvard University Press. be applied to a diverse range of functional domains such as move- Copyright 2017 by the President and Fellows of Harvard College. All ment control, sensory processing, language, pain, and cognition. For rights reserved. example, recent randomized controlled clinical trials for motor recov- Loscalzo J et al: Human disease classification in the postgenomic era: ery after stroke have suggested that intensity of training may be par- A complex systems approach to human pathobiology. Mol Syst Biol ticularly important for sustained long-term improvements. Moreover, 3:124, 2007. studies of the effects of such training in rodent and nonhuman primate Maiorino E, Loscalzo J: Phenomics and robust multiomics data models further suggest that plasticity of cortical “motor maps” as well for cardiovascular disease subtyping. Arterioscl Thromb Vasc Biol as the coordinated firing of neurons in remaining networks underlie 43:1111, 2023. observed functional improvements with rehabilitation. The incorpora- Menche J et al: Disease networks. Uncovering disease-disease rela- tion of technology for neurologic rehabilitation has the great potential tionships through the incomplete interactome. Science 347:1257601, to revolutionize the delivery of care by significantly increasing access, 2015. reducing the burden for adherence to high-intensity regimens, and Oldham WM et al: Network analysis to risk stratify patients with exer- maximizing engagement. Below are three examples of how emerging cise intolerance. Circ Res 122:864, 2018. technology can be used to harness neural plasticity and maximize Paci P et al: Gene co-expression in the interactome: Moving from functional restoration. correlation toward causation via an integrated approach to disease module discovery. NPJ Syst Biol App 7:3, 2021. ■ ROBOTICS Wang R et al: Multiomics network medicine approaches to precision Rehabilitation robotics for both the upper and the lower limb have medicine and therapeutics in cardiovascular diseases Arterioscl the potential to improve motor outcomes after stroke or other forms Thromb Vasc Biol 43:493, 2023. of brain injury. There is a growing recognition that focused training involving a range of tasks might be important for improved functional outcomes. While there is a growing recognition of “sensitive periods” that might represent optimal windows for rehabilitation after injury (e.g., perhaps the first several months after a stroke), such training likely has a role in the chronic period as well (e.g., maintenance therapy may also guard against known declines in function over time). Notably, the delivery of intensive training is a great challenge from both the per- 500 Emerging Neurotherapeutic spective of the health care system and each patient. Outside of clinical Technologies trials, such a training program can be quite difficult to implement and maintain. It can also be costly and require significant effort. Motor rehabilitation protocols using robotics have been developed Jyoti Mishra, Karunesh Ganguly and tested for both the upper limb and the lower limb. Such robotic therapies have often focused on the delivery of high-intensity move- ment practice that can surpass what is possible via existing standards Neurotherapeutic technologies represent a diverse group of very of care. Moreover, robotic systems are capable of precisely measuring promising treatment approaches with a common purpose of improving movement parameters (e.g., the kinematics of the movements) and neurologic function. Decades of basic science research have paved the providing quantitative feedback regarding the changes in performance path for these novel technologies that have the potential to transform during the training period. A particular focus has been on maximizing the lives of patients with neurologic diseases. A key goal is to minimize patient engagement and recruitment of attentional and reward path- the consequences of lost abilities, whether they are motor, sensory, or ways, both of which are increasingly recognized to drive neural plastic- cognitive. A common objective is to also harness the inherent plastic- ity. Ongoing advances in design and the user interface will continue to ity of the nervous system, regardless of age, and even in the face of a improve comfort and support sustained effort. For example, via close degenerative process. monitoring of performance and movement parameters, the system The technologies described below are the culmination of both an can aid at key points in order to minimize fatigue and ensure maximal increased understanding of neural plasticity mechanisms in both the engagement. Moreover, antigravity support of the upper limb can allow intact and the injured nervous system as well as advances in technol- practice and task engagement even in the presence of severe weakness; ogy and computational power. While it is also clear that there may be this would be extremely challenging and labor intensive under current fundamental limits on plasticity and repair mechanisms (the closing of standards of care. Recent analysis also suggests that robotic devices developmental windows and/or loss of the ability of a network to com- may at least match outcomes realized with existing standards of care. pensate), the brain remains highly plastic regardless of age and even in However, rehabilitation robotics may also provide more precise feed- the face of ongoing injury and/or degenerative processes. Collectively, back and permit novel quantitative rehabilitation approaches. there is now growing evidence to support neurologic restorative efforts Figure 500-1 shows one example of an upper-limb robotic exoskel- for both “static” (e.g., stroke) and progressive neurologic disorders. eton device that is currently being evaluated for training after stroke. These technologies may not appear, at first glance, directly relevant A randomized, multicenter trial compared treatment with this exo- to traditional medical care, but it is worth noting that clinicians have skeleton system against conventional therapy provided by physical and the most knowledge and experience about specific disease processes, occupational therapists. Participants were enrolled in the chronic phase available treatments, and the expected course of illnesses affecting and all had moderate-to-severe deficits; the groups underwent three the nervous system. It is thus critical that neurologic specialists and sessions per week over an 8-week period. For robotic training, subjects other clinicians play an important role in the future adoption of these trained with games to improve mobilization and to practice activities of technologies for neurologic rehabilitation. The sections below outline daily living. This study provided evidence that both conventional and
[PAGE 3964] 3964 PART 20 Emerging Topics in Clinical Medicine enhanced view of the world around. AR is being tested in a diverse group of patients with neurologic impairments in the motor,
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: Figure 500-1 shows one example of an upper-limb robotic exoskel- eton device that is currently being evaluated for training after stroke. A randomized, multicenter trial compared treatment with this exo- skeleton system against conventional therapy provided by physical and occupational therapists. Participants were enrolled in the chronic phase and all had moderate-to-severe deficits; the groups underwent three sessions per week over an 8-week period. For robotic training, subjects trained with games to improve mobilization and to practice activities of daily living. This study provided evidence that both conventional and
Figure 2¶
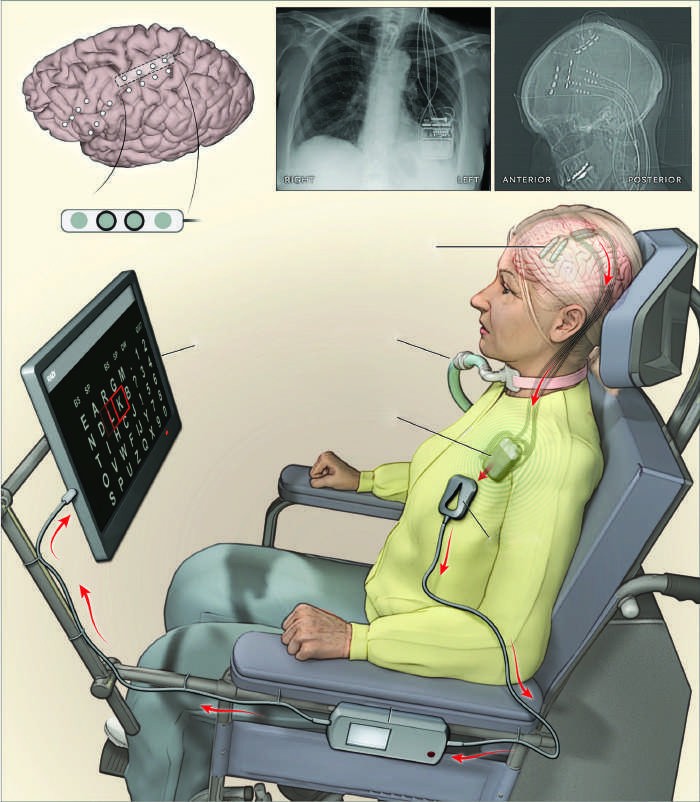
Caption: FIGURE 500-6 Illustration of an amyotrophic lateral sclerosis (ALS) patient with a fully the brain. B. X-ray of chest showing the wireless module. C. X-ray of leads and wire et al: Fully implanted brain–computer interface in a locked-in patient with ALS. N Engl J with permission from Massachusetts Medical Society.)
Figure 3¶

Caption: FIGURE 500-2 Augmented reality (AR) for phantom limb pain. A. A patient is shown a live activation during training. C. The patient matches target postures during rehabilitation. (M Ortiz-Catalan et al: Phantom motor execution facilitated by machine learning and patients with chronic intractable phantom limb pain. Lancet 388:2885, 2016.)
Figure 4¶
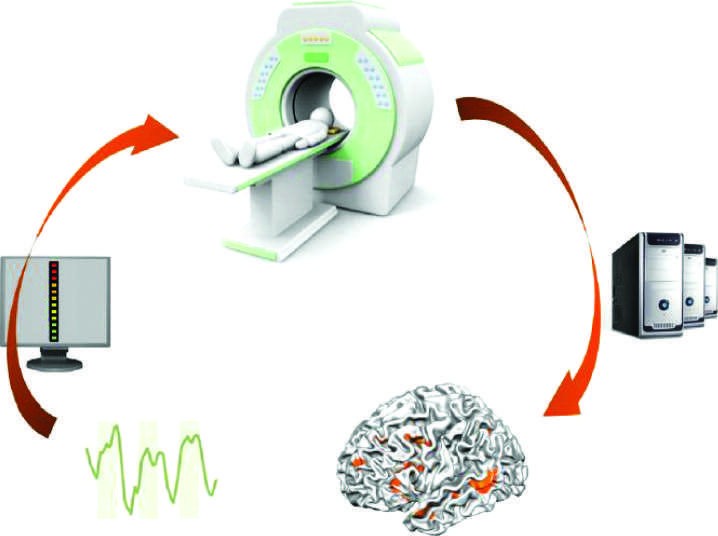
Caption: FIGURE 500-3 Neurofeedback using functional magnetic resonance imaging (fMRI). neurocognitive models of auditory-visual hallucinations into therapy. Front Psychiatry
Figure 5¶

Caption: FIGURE 500-2 Augmented reality (AR) for phantom limb pain. A. A patient is shown a live activation during training. C. The patient matches target postures during rehabilitation. (M Ortiz-Catalan et al: Phantom motor execution facilitated by machine learning and patients with chronic intractable phantom limb pain. Lancet 388:2885, 2016.)
Figure 6¶

Caption: FIGURE 500-2 Augmented reality (AR) for phantom limb pain. A. A patient is shown a live activation during training. C. The patient matches target postures during rehabilitation. (M Ortiz-Catalan et al: Phantom motor execution facilitated by machine learning and patients with chronic intractable phantom limb pain. Lancet 388:2885, 2016.)
Figure 7¶

Caption: FIGURE 500-1 Photograph of a subject interacting with a complex upper-limb to enhance visual feedback during gait training. exoskeleton and a virtual reality system. (From U Keller et al: Robot-assisted arm assessments in spinal cord injured patients: A consideration of concept study. PLoS Figure 500-2 shows an innovative application of AR for the treat- One 10:e0126948, 2015.) ment of “phantom limb” pain. A subset of both upper-limb and lower- limb amputees experience painful sensations that appear to originate from the missing limb. Past research has suggested that mirror therapy robotic therapy could improve function in patients with chronic stroke. can be an effective treatment for phantom limb pain. During mir- Multiple studies have also found similar gains when using either con- ror therapy treatments, patients move their healthy arm in front of ventional or traditional approaches. Thus, a growing body of research a mirror to produce a perception of movements of the missing limb.
Figure 8¶

Caption: FIGURE 500-2 Augmented reality (AR) for phantom limb pain. A. A patient is shown a live activation during training. C. The patient matches target postures during rehabilitation. (M Ortiz-Catalan et al: Phantom motor execution facilitated by machine learning and patients with chronic intractable phantom limb pain. Lancet 388:2885, 2016.)
Figure 9¶

Caption: FIGURE 500-4 Illustration of transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS) setups. The upper panels show a TMS setup. Coils generate magnetic fields that can in turn generate electrical fields in the cortical tissue. The lower panels show a tDCS setup. The electrical current is believed to flow from the anode (+) to the cathode (–) through the superficial cortical areas leading to polarization. (Reproduced with permission from R Sparing, FM Mottaghy: Noninvasive brain stimulation with transcranial magnetic or direct current stimulation [TMS/tDCS]—From insights into human memory to therapy of its dysfunction. Methods 44:329, 2008.)
Figure 10¶

Caption: a FIGURE 500-5 Components of a brain–machine interface (BMI). (Reproduced with A Tsu et al: Cortical neuroprosthetics from a clinical perspective. Neurobiol Dis 83:154, to each individual are lacking. BCIs offer a promising means to restore through patient groups described above, while the pathways for Recent studies of signals to muscles are disrupted, the brain itself is largely patterns of net- Thus, BCIs can restore function by communicating how the patient brain. For example, in a “motor” BCI, a subject’s intention studies that aim translated in real time to control a device. As illustrated in the components of a motor BCI include the following: (1)
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.