Dilated Cardiomyopathies¶
Chapter 269 | Part 6: Disorders of the Cardiovascular System · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Alcoholic cardiomyopathy requires cessation of alcohol; 3–4 ounces of pure ethanol daily for ≥5 years is the estimated threshold, though women may develop it with lower amounts.
- Peripartum cardiomyopathy (PPCM) recovery to LVEF ≥0.50 occurs in 50–80% of cases within 6 months; recovery is less likely with LVEF 6 weeks after delivery.
- Anthracycline cardiotoxicity is managed with beta-adrenergic blockade and RAAS inhibition; dexrazoxane may prevent toxicity but consensus on timing is lacking.
- Takotsubo syndrome (stress-induced cardiomyopathy) typically resolves within days to weeks; recurrence occurs in 10% of patients at an estimated rate of 2%/year.
- Checkpoint inhibitor myocarditis requires immediate high-dose glucocorticoids; outcomes are improving with earlier recognition and therapy.
- Hemochromatosis diagnosis is made principally by MRI iron quantitation; phlebotomy is the management for early disease to remove iron.
- Trastuzumab cardiomyopathy may persist in about a third of affected patients and can progress to clinical heart failure and death.
- PPCM anticoagulation is usually prescribed for the first 6 weeks postpartum if LVEF <0.35 or marked dilation is present due to thrombus risk.
- TTN truncating mutations are found in ~15% of PPCM cases and are associated with lower rates of recovered systolic function.
- Vaccine-induced myocarditis risk after COVID-19 vaccines is estimated at 1/100,000 doses, increasing to 2–3/100,000 for recipients age 18–39 years.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Pathophysiology of Progression
- 2. EPIDEMIOLOGY
- 2.1 Alcohol-Related Epidemiology
- 2.2 Peripartum Cardiomyopathy Epidemiology
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Infective Myocarditis
- 3.2 Noninfective Inflammatory Disease
- 3.3 Toxic Causes
- 3.4 Metabolic Causes
- 3.5 Miscellaneous Causes
- 4. CLINICAL FEATURES
- 4.1 Peripartum Cardiomyopathy Presentation
- 4.2 Takotsubo Syndrome Presentation
- 4.3 Metabolic and Nutritional Presentation
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Alcohol vs. Genetic Cardiomyopathy
- 5.2 Takotsubo vs. Acute MI
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria for PPCM
- 6.2 Diagnostic Criteria for Hemochromatosis
- 6.3 Diagnostic Criteria for Takotsubo Syndrome
- 7. MANAGEMENT & TREATMENT
- 7.1 Management of Anthracycline Cardiotoxicity
- 7.2 Management of Peripartum Cardiomyopathy
- 7.3 Management of Takotsubo Syndrome
- 7.4 Management of Hemochromatosis
- 7.5 Management of Pheochromocytoma
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 PPCM Prognostic Factors
- 8.2 Takotsubo Prognosis
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy and Breastfeeding
- 9.2 Pediatric Considerations
- 9.3 Nutritional Deficiencies
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Pitfalls
- 10.2 Treatment Traps
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Hemochromatosis |
| 2 | 🖼 Figure | Hemochromatosis |
| 3 | 🖼 Figure | Hemochromatosis |
| 4 | 🖼 Figure | Figure / Illustration |
1. DEFINITION & OVERVIEW¶
- Dilated cardiomyopathy (DCM) is characterized by decreased left ventricular systolic function, typically with increased left ventricular dimensions, although dilation may be minimal in some cases.
- Despite multiple etiologies and variable initial presentations, DCM often progresses into a convergent clinical phenotype similar to that of other injury such as acute myocardial infarction.
- Some myocytes may die early in the course, while others survive only to have later programmed cell death (apoptosis), and remaining myocytes develop hypertrophy in response to increased wall stress.
- Local and circulating neurohormonal factors stimulate deleterious secondary responses that contribute to progression of disease.
- Dynamic remodeling of the interstitial scaffolding affects diastolic function and the amount of ventricular dilation.
- Mitral regurgitation commonly develops as the ventricle dilates and the valvular apparatus is distorted and is commonly moderate to severe by the time heart failure is advanced.
- Dilation and decreased function of the right ventricle may result directly from the initial injury but more often develop later in response to elevated afterload presented by secondary pulmonary hypertension and in relation to mechanical interactions with the failing left ventricle.
- The secondary responses are often modifiable or reversible. Almost a third of patients with recent-onset cardiomyopathy in the absence of coronary artery disease demonstrate substantial spontaneous recovery to normal ejection fraction.
- Partial recovery to left ventricular ejection fraction (LVEF) >0.40 is common in chronic DCM during recommended therapy with neurohormonal modulation, cardiac resynchronization therapy for left bundle branch block, and diuretics as needed to maintain fluid balance.
1.1 Pathophysiology of Progression¶
- Myocyte death occurs early in the course, while others survive only to have later programmed cell death (apoptosis).
- Remaining myocytes develop hypertrophy in response to increased wall stress.
- Local and circulating neurohormonal factors stimulate deleterious secondary responses that contribute to progression of disease.
- Dynamic remodeling of the interstitial scaffolding affects diastolic function and the amount of ventricular dilation.
- Mitral regurgitation commonly develops as the ventricle dilates and the valvular apparatus is distorted.
- Dilation and decreased function of the right ventricle may result directly from the initial injury but more often develop later in response to elevated afterload presented by secondary pulmonary hypertension and in relation to mechanical interactions with the failing left ventricle.
2. EPIDEMIOLOGY¶
- Alcoholic cardiomyopathy causes many more hospital admissions in men than women, but prevalence is similar between men and women with alcoholism.
- Left ventricular dysfunction is detected in about a third of asymptomatic patients with alcoholism.
- Estimates of the alcohol intake necessary to cause cardiomyopathy have been 3–4 ounces or ≥60–80 g of pure ethanol daily for ≥5 years, about 750 mL of wine, 6 beers, or a half pint of hard liquor.
- Women may develop cardiomyopathy with lower amounts of consumption.
- Frequent binge drinking may also be sufficient.
- Peripartum cardiomyopathy (PPCM) affects between 1:1000 and 1:4000 deliveries in the United States.
- Risk of PPCM is fourfold higher in black women, in whom recovery of normal LVEF takes longer and is less likely than in white women.
- One-year mortality rates after PPCM have ranged in the United States from 4% in one study to 11% in a population of black women, and have been reported as up to twofold higher in Africa.
2.1 Alcohol-Related Epidemiology¶
- Alcoholic cardiomyopathy causes many more hospital admissions in men than women.
- Prevalence is similar between men and women with alcoholism.
- Left ventricular dysfunction is detected in about a third of asymptomatic patients with alcoholism.
- Estimates of the alcohol intake necessary to cause cardiomyopathy have been 3–4 ounces or ≥60–80 g of pure ethanol daily for ≥5 years.
- Women may develop cardiomyopathy with lower amounts of consumption.
- Frequent binge drinking may also be sufficient.
2.2 Peripartum Cardiomyopathy Epidemiology¶
- PPCM affects between 1:1000 and 1:4000 deliveries in the United States.
- Risk of PPCM is fourfold higher in black women.
- Recovery of normal LVEF takes longer and is less likely in black women than in white women.
- One-year mortality rates after PPCM have ranged in the United States from 4% to 11%.
- Mortality rates have been reported as up to twofold higher in Africa.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Multiple causes and contributing factors have been implicated (Table 269-1).
- Many cases are attributed to prior myocarditis, and an increasing number are associated with pathogenic genetic variants.
- Other causes include toxic and metabolic disorders and peripartum cardiomyopathy.
- Vaccines have occasionally been implicated in myocarditis, particularly after the smallpox vaccine in military populations and more recently with COVID-19 vaccines.
- The most dramatic form of noninfectious inflammatory myocarditis is that seen with combined immune checkpoint inhibitors.
- Cardiotoxicity has been reported with multiple environmental and pharmacologic agents.
- Chemotherapy agents are the most common drugs implicated in toxic cardiomyopathy.
- Vascular endothelial growth factor (VEGF), produced endogenously or by tumors, enhances angiogenesis by activating the VEGF signaling pathways.
- Monoclonal antibodies and many small-molecule tyrosine kinase inhibitors that affect VEGF are in use for different malignancies.
- Blood pressures increase in most patients during therapy, attributed to an imbalance between endogenous vasodilators and vasoconstrictors and alteration of glomerular function.
- Hypertension and proteinuria can develop with these agents, similar to preeclampsia, and presentation is associated with increased risk of future cardiac disease.
- Hemochromatosis is variably classified as a metabolic or storage disease.
- The autosomal recessive form is related to the HFE gene.
- Cardiac siderosis can also be acquired from iron overload due to hemoglobinopathies in patients treated with recurrent transfusions.
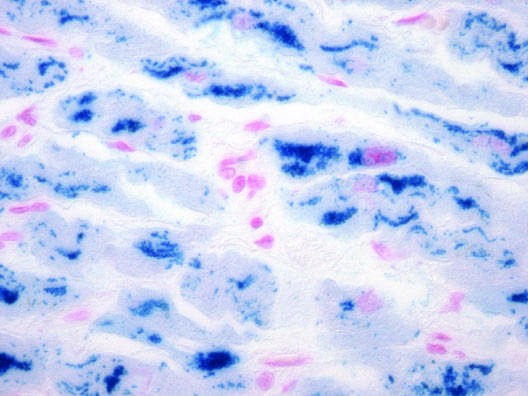
- Excess iron is deposited in the perinuclear compartment of cardiomyocytes, with resulting disruption of intracellular architecture and mitochondrial function.
Table 1 — Table 269-1 Major Causes of Dilated Cardiomyopathy (with Common Examples)¶
| Category | Specific Causes |
|---|---|
| Inflammatory Myocarditis (see Chap. 268) | Infective: Viral (coxsackie, adenovirus, COVID-19, HIV); Parasitic (Trypanosoma cruzi—Chagas' disease, trypanosomiasis, toxoplasmosis); Bacterial (diphtheria); Spirochetal (Borrelia burgdorferi—Lyme disease); Rickettsial (Q fever); Fungal (with systemic infection) |
| Noninfective | Granulomatous inflammatory disease; Sarcoidosis; Giant cell myocarditis; Eosinophilic myocarditis; Polymyositis, dermatomyositis; Collagen vascular disease; Checkpoint inhibitor chemotherapy; Transplant rejection |
| Toxic | Alcohol; Catecholamines: amphetamines, cocaine; Chemotherapeutic agents (anthracyclines, trastuzumab); Interferon; Other therapeutic agents (hydroxychloroquine, chloroquine); Drugs of misuse (testosterone and other anabolic steroids, emetine); Heavy metals: lead, mercury; Occupational exposure: hydrocarbons, arsenicals |
| Metabolic | Nutritional deficiencies: thiamine, selenium, carnitine; Electrolyte deficiencies: calcium, phosphate, magnesium; Endocrinopathy: Thyroid disease, Pheochromocytoma, Diabetes mellitus, Obesity, Hemochromatosis; Inherited metabolic pathway defects (see Chap. 267); Familial (see Table 267-1) |
| Cardiomyopathies without extracardiac involvement | Cardiomyopathy with skeletal myopathy, for example: Dystrophin-related dystrophy (Duchenne's, Becker's); Mitochondrial myopathies (e.g., Kearns-Sayre syndrome); Hemochromatosis; Susceptibility to immune-mediated myocarditis |
| Associated with other systemic diseases | Miscellaneous (Shared Elements of Above Etiologies): Arrhythmogenic ventricular cardiomyopathy; Peripartum cardiomyopathy; Left ventricular noncompaction; Tachycardia-related cardiomyopathy; Supraventricular arrhythmias with uncontrolled rate; Very frequent nonsustained ventricular tachycardia or high burden of premature ventricular complexes |
3.1 Infective Myocarditis¶
- Viral (coxsackie, adenovirus, COVID-19, HIV).
- Parasitic (Trypanosoma cruzi—Chagas' disease, trypanosomiasis, toxoplasmosis).
- Bacterial (diphtheria).
- Spirochetal (Borrelia burgdorferi—Lyme disease).
- Rickettsial (Q fever).
- Fungal (with systemic infection).
3.2 Noninfective Inflammatory Disease¶
- Granulomatous inflammatory disease.
- Sarcoidosis.
- Giant cell myocarditis.
- Eosinophilic myocarditis.
- Polymyositis, dermatomyositis.
- Collagen vascular disease.
- Checkpoint inhibitor chemotherapy.
- Transplant rejection.
3.3 Toxic Causes¶
- Alcohol.
- Catecholamines: amphetamines, cocaine.
- Chemotherapeutic agents (anthracyclines, trastuzumab).
- Interferon.
- Other therapeutic agents (hydroxychloroquine, chloroquine).
- Drugs of misuse (testosterone and other anabolic steroids, emetine).
- Heavy metals: lead, mercury.
- Occupational exposure: hydrocarbons, arsenicals.
3.4 Metabolic Causes¶
- Nutritional deficiencies: thiamine, selenium, carnitine.
- Electrolyte deficiencies: calcium, phosphate, magnesium.
- Endocrinopathy: Thyroid disease, Pheochromocytoma, Diabetes mellitus, Obesity, Hemochromatosis.
- Inherited metabolic pathway defects.
- Familial cardiomyopathies.
3.5 Miscellaneous Causes¶
- Arrhythmogenic ventricular cardiomyopathy.
- Peripartum cardiomyopathy.
- Left ventricular noncompaction.
- Tachycardia-related cardiomyopathy.
- Supraventricular arrhythmias with uncontrolled rate.
- Very frequent nonsustained ventricular tachycardia or high burden of premature ventricular complexes.
4. CLINICAL FEATURES¶
- Presentations include pulmonary edema, hypotension, and chest pain with electrocardiogram (ECG) changes mimicking an acute infarction.
- The left ventricular dysfunction extends beyond a specific coronary artery distribution and generally resolves within days to weeks.
- Most cases of PPCM present within the first week after delivery, usually with increasing edema and dyspnea when urine output does not keep up with mobilization of fluid.
- Both atrial and ventricular arrhythmias can occur.
- It is important to exclude other complications of pregnancy such as pulmonary emboli and coronary artery dissection.
- Patients with pheochromocytoma often have postural hypotension.
- In addition to alpha-adrenergic receptor antagonists, definitive therapy requires surgical extirpation for pheochromocytoma.
- Very high renin states, such as those caused by renal artery stenosis, can lead to modest depression in ejection fraction with little or no ventricular dilation and markedly labile symptoms with flash pulmonary edema, related to sudden shifts in vascular tone and intravascular volume.
- Controversies remain regarding whether diabetes mellitus and obesity are sufficient to cause cardiomyopathy with reduced ejection fraction.
- Most heart failure in diabetes mellitus results from epicardial coronary disease, with further increase in coronary artery risk due to accompanying hypertension and renal dysfunction.
- Cardiomyopathy may result in part from insulin resistance and increased advanced-glycosylation end products, which impair both systolic and diastolic function.
- However, much of the dysfunction can be attributed to scattered focal ischemia resulting from distal coronary artery tapering and limited microvascular perfusion even without proximal focal stenoses.
- Diabetes mellitus is a typical factor in heart failure with 'preserved' ejection fraction, along with hypertension, advanced age, and female gender.
- The existence of a cardiomyopathy due to obesity is generally accepted, but the overlap is not well defined with the syndrome of heart failure with preserved ejection fraction (HFpEF).
- In addition to cardiac involvement from associated diabetes mellitus, hypertension, and vascular inflammation of the metabolic syndrome, obesity alone is associated with impaired excretion of excess volume load, which, over time, can lead to increased wall stress and secondary adaptive neurohormoral responses.
- Fluid retention may be aggravated by large fluid intake and the rapid clearance of natriuretic peptides by adipose tissue.
- In the absence of another obvious cause of cardiomyopathy in an obese patient with systolic dysfunction without marked ventricular dilation, effective weight reduction is often associated with major improvement in ejection fraction and clinical function.
- Improvement in cardiac function has been described after successful bariatric surgery, although all major surgical therapy poses increased risk for patients with heart failure.
- Postoperative malabsorption and nutritional deficiencies, such as calcium and phosphate deficiencies, may be particularly deleterious for patients with cardiomyopathy.
- Nutritional deficiencies can occasionally cause DCM but are not commonly implicated in developed countries.
- Beriberi heart disease due to thiamine deficiency can result from poor nutrition in undernourished populations and in patients deriving most of their calories from alcohol and has been reported in teenagers subsisting only on highly processed foods.
- This disease is initially a vasodilated state with very-high-output heart failure that can later progress to a low-output state; thiamine repletion can lead to prompt recovery of cardiovascular function.
- Abnormalities in carnitine metabolism can cause dilated or restrictive cardiomyopathies, usually in children.
- Deficiency of trace elements such as selenium can cause cardiomyopathy (Keshan's disease).
- Calcium is essential for excitation-contraction coupling.
- Chronic deficiencies of calcium, such as can occur with hypoparathyroidism (particularly postsurgical) or intestinal dysfunction (from diarrheal syndromes and following extensive resection), can cause severe chronic heart failure that responds over days or weeks to vigorous calcium repletion.
- Phosphate is a component of high-energy compounds needed for efficient energy transfer and multiple signaling pathways.
- Hypophosphatemia can develop during starvation and early refeeding following a prolonged fast and occasionally during hyperalimentation.
4.1 Peripartum Cardiomyopathy Presentation¶
- PPCM develops during the last trimester or within the first 5–6 months after pregnancy, most commonly within the first 2 weeks after delivery.
- Most cases of PPCM present within the first week after delivery.
- Presentation includes increasing edema and dyspnea when urine output does not keep up with mobilization of fluid.
- Both atrial and ventricular arrhythmias can occur.
- It is important to exclude other complications of pregnancy such as pulmonary emboli and coronary artery dissection.
4.2 Takotsubo Syndrome Presentation¶
- Apical ballooning or 'takotsubo' syndrome, also referred to as stress-induced cardiomyopathy or 'broken heart syndrome'.
- It occurs typically in older women after sudden intense emotional or physical stress.
- The ventricle shows global ventricular dilation with basal contraction, forming the shape of the narrow-necked jar (takotsubo) used in Japan to trap octopuses.
- Presentations include pulmonary edema, hypotension, and chest pain with electrocardiogram (ECG) changes mimicking an acute infarction.
- The left ventricular dysfunction extends beyond a specific coronary artery distribution and generally resolves within days to weeks.
4.3 Metabolic and Nutritional Presentation¶
- Beriberi heart disease due to thiamine deficiency is initially a vasodilated state with very-high-output heart failure that can later progress to a low-output state.
- Thiamine repletion can lead to prompt recovery of cardiovascular function.
- Abnormalities in carnitine metabolism can cause dilated or restrictive cardiomyopathies, usually in children.
- Deficiency of trace elements such as selenium can cause cardiomyopathy (Keshan's disease).
- Chronic deficiencies of calcium can cause severe chronic heart failure that responds over days or weeks to vigorous calcium repletion.
- Hypophosphatemia can develop during starvation and early refeeding following a prolonged fast and occasionally during hyperalimentation.
5. DIFFERENTIAL DIAGNOSIS¶
- Dilated cardiomyopathy is often a diagnosis of exclusion for toxic causes like alcohol.
- Alcoholic cardiomyopathy remains a diagnosis of exclusion.
- Mendelian randomization studies have not identified a link between genetically predicated alcohol consumption and heart failure, suggesting that the population attributable risk of alcohol to the overall heart failure epidemic is modest.
- Controversies remain regarding whether diabetes mellitus and obesity are sufficient to cause cardiomyopathy with reduced ejection fraction.
- Most heart failure in diabetes mellitus results from epicardial coronary disease, with further increase in coronary artery risk due to accompanying hypertension and renal dysfunction.
- The existence of a cardiomyopathy due to obesity is generally accepted, but the overlap is not well defined with the syndrome of heart failure with preserved ejection fraction (HFpEF).
- In the absence of another obvious cause of cardiomyopathy in an obese patient with systolic dysfunction without marked ventricular dilation, effective weight reduction is often associated with major improvement in ejection fraction and clinical function.
- Takotsubo syndrome is distinguished from acute myocardial infarction by the resolution of dysfunction within days to weeks and the absence of coronary artery occlusion.
- Coronary angiography may be required to rule out acute coronary occlusion in Takotsubo syndrome.
- A diagnosis of systemic iron overload is made from measurement of serum iron and transferrin saturation, with a threshold of >60% for men and >45–50% for women.
- MRI is used to quantitate iron stores in the liver and heart.
- While endomyocardial biopsy tissue can be stained for iron, a diagnosis of cardiac iron overload is made principally by MRI and biopsy is not usually needed.
5.1 Alcohol vs. Genetic Cardiomyopathy¶
- Alcoholic cardiomyopathy remains a diagnosis of exclusion.
- Mendelian randomization studies have not identified a link between genetically predicated alcohol consumption and heart failure.
- Mutations in TTN and other DCM disease genes can be identified in ~10% of patients with presumed alcohol cardiomyopathy.
5.2 Takotsubo vs. Acute MI¶
- Takotsubo syndrome is distinguished from acute myocardial infarction by the resolution of dysfunction within days to weeks.
- Coronary angiography may be required to rule out acute coronary occlusion in Takotsubo syndrome.
- The left ventricular dysfunction extends beyond a specific coronary artery distribution.
6. INVESTIGATIONS & DIAGNOSIS¶
- Echocardiography may suggest myocardial edema, but initial ejection fraction may not be markedly reduced.
- Initial care should generally not be delayed for endomyocardial biopsy, which typically shows extensive lymphocytic infiltration.
- Patients may also present initially with other acute organ system involvement, which warrants urgent multidisciplinary management in intensive care.
- Therapy with high-dose glucocorticoids should be initiated rapidly and may be followed soon by more targeted immune inhibition.
- Reports of fatality in checkpoint inhibition myocarditis were initially very high, but outcomes are improving with earlier recognition and therapy.
- Echocardiography is usually sufficient for diagnosis of PPCM, but in complex cases, cardiac magnetic resonance imaging (MRI) can be considered, but gadolinium should not be used.
- MRI is used to quantitate iron stores in the liver and heart.
- A diagnosis of cardiac iron overload is made principally by MRI and biopsy is not usually needed.
- A diagnosis of systemic iron overload is made from measurement of serum iron and transferrin saturation, with a threshold of >60% for men and >45–50% for women.
- While endomyocardial biopsy tissue can be stained for iron, a diagnosis of cardiac iron overload is made principally by MRI and biopsy is not usually needed.
- Genetic testing should be considered as the results may impact the mother, in whom positive genetic testing predicts less recovery, and also other family members, too.
- Diagnosis of cardiomyopathy secondary to cobalt toxicity may be secondary to impaired myocardial energetics and is more common in the setting of hypothyroidism and dietary protein and thiamine deficiency.
- Cobalt cardiomyopathy usually presents with polycythemia, hypothyroidism, and goiter due to the effects of cobalt on red cell production and thyroxine.
- Diagnosis occurs in the setting of cobalt exposure and can be confirmed by the presence of electron microscopy dense intramitochondrial particles.
6.1 Diagnostic Criteria for PPCM¶
- PPCM usually presents with evidence of congestion.
- Criteria generally include an LVEF ≤0.45 presenting toward the end of pregnancy in the absence of another cardiac diagnosis.
- Elevated levels of natriuretic peptides, troponin, and sFLT1 have also been associated with less recovery.
6.2 Diagnostic Criteria for Hemochromatosis¶
- A diagnosis of systemic iron overload is made from measurement of serum iron and transferrin saturation.
- Threshold of >60% for men and >45–50% for women.
- MRI is used to quantitate iron stores in the liver and heart.
- While endomyocardial biopsy tissue can be stained for iron, a diagnosis of cardiac iron overload is made principally by MRI and biopsy is not usually needed.
6.3 Diagnostic Criteria for Takotsubo Syndrome¶
- Ventricle shows global ventricular dilation with basal contraction, forming the shape of the narrow-necked jar (takotsubo).
- Coronary angiography may be required to rule out acute coronary occlusion.
- Cardiac MRI demonstrates diffuse myocardial edema without necrosis and abnormal myocardial calcium handling.
- ECG changes mimicking an acute infarction.
7. MANAGEMENT & TREATMENT¶
- Therapy includes conventional guideline-directed medical therapies with neurohormonal, mineralocorticoid receptor, and beta-adrenergic antagonists as well as sodium-glucose cotransporter 2 inhibitors with diuretics as needed for fluid management and careful attention to electrolyte repletion.
- Withdrawal should be supervised to avoid exacerbations of heart failure or arrhythmias and ongoing support arranged.
- Even with severe disease, marked improvement can occur within 3–6 months of abstinence, but the prognosis is grim if heavy alcohol consumption continues.
- Therapy for reduced ejection fraction due to anthracycline therapy includes beta-adrenergic receptor blockade and inhibition of the renin-angiotensin system, with conflicting data on whether these agents decrease toxicity when given in parallel with chemotherapy.
- The use of dexrazoxane, an intracellular iron chelating agent, can prevent anthracycline cardiomyopathy, but there is no consensus on when it should be used owing to concerns that it might attenuate the efficacy of cancer therapies.
- Therapeutic approaches include management of associated hypertension, withdrawal of the tyrosine kinase inhibitor (when possible), and conventional treatment for heart failure.
- Newer tyrosine kinase inhibitors effective against multiple kinases may have more complex off-target effects.
- This includes the Bruton tyrosine kinase inhibitors (e.g., ibrutinib), which are used as primary therapy for lymphoid malignancies, with predominant cardiovascular risks of atrial and ventricular arrhythmias in addition to heart failure.
- Proteasome inhibitors used to treat multiple myeloma are associated with an increased risk of hypertension, ischemic events, thromboembolism, and heart failure.
- The more potent agent, carfilzomib, appears more cardiotoxic than bortezomib.
- Other treatments for myeloma include immunomodulatory drugs including lenalidomide and thalidomide, which may cause heart failure in addition to risks of venous thromboembolism.
- Mitogen-activated extracellular signal regulated kinase (MEK) inhibitors used for metastatic melanoma may cause brain hypertension and cardiomyopathy, especially when co-administered with rapidly accelerated fibrosarcoma (RAF) inhibitors.
- Recognition of cardiotoxicity during therapy with these agents is complicated because they occasionally cause peripheral fluid accumulation (ankle edema, periorbital swelling, pleural effusions) due to local factors rather than elevated central venous pressures.
- Therapeutic approaches include management of associated hypertension, withdrawal of the tyrosine kinase inhibitor (when possible), and conventional treatment for heart failure.
- Initial treatment for PPCM includes loop diuretics as needed to restore normal volume status.
- Prior to delivery, close collaboration with the maternal-fetal medicine team is necessary to adjust therapies to stabilize the gravid mother while protecting the fetus.
- Digoxin and beta blockers can be used if needed for arrhythmias, and hydralazine/nitrate combinations can be used for hypertension, but renin-angiotensin system inhibitors should not be given due to adverse fetal effects.
- Hemodynamic instability may require ongoing hemodynamic monitoring, and plans should be in place for emergency delivery if necessary.
- When the mother is hemodynamically stable in the postpartum period, metoprolol tartrate, enalapril, and spironolactone have been shown to be compatible with breastfeeding.
- PPCM with LVEF <0.35 or marked dilation carries increased incidence of left ventricular thrombus and embolic risk, so anticoagulation is usually prescribed for the first 6 weeks once obstetric bleeding has resolved.
- Breastfeeding was once prohibited but now is generally encouraged in patients in whom fluid balance can be maintained through the high oral fluid intake required.
- For patients who are not breastfeeding, there is an ongoing large, randomized trial to determine the impact of bromocriptine on PPCM outcomes.
- For cardiotoxicity with anthracyclines or trastuzumab, therapy is recommended as for other causes of reduced ejection fraction.
- For cardiotoxicity with cyclophosphamide and ifosfamide, generally occurs acutely and with very high doses.
- 5-Fluorouracil, cisplatin, and some other alkylating agents can cause recurrent coronary spasm that occasionally leads to depressed contractility.
- Acute administration of interferon-alpha, interleukin 2, and other cytokine-based therapies can cause pericarditis, hypotension, and arrhythmias.
- Clinical heart failure occurring during their chronic administration usually resolves after discontinuation.
- Treatment for these disorders includes removing exposure to the toxin and standard medical therapy for heart failure with reduced ejection fraction.
- Cardiomyopathy secondary to cobalt toxicity may be secondary to impaired myocardial energetics and is more common in the setting of hypothyroidism and dietary protein and thiamine deficiency.
- Treatment for these disorders includes removing exposure to the toxin and standard medical therapy for heart failure with reduced ejection fraction.
- If diagnosed early, hemochromatosis can often be managed by repeated phlebotomy to remove iron.
- For more severe iron overload, iron chelation therapy with desferrioxamine (deferoxamine) or deferasirox can help to improve cardiac function if myocyte loss and replacement fibrosis are not too severe.
- No therapies have been proven beneficial for Takotsubo syndrome, but reasonable strategies include nitrates for pulmonary edema; combined alpha and beta blockers rather than selective beta blockade if hemodynamically stable; and magnesium for arrhythmias related to QT prolongation.
- An intra-aortic balloon pump is occasionally employed to improve critically low cardiac output, but only if there is no left ventricular outflow tract obstruction.
- Hyperthyroidism should always be considered with new-onset atrial fibrillation or ventricular tachycardia or atrial fibrillation in which the rapid ventricular response is difficult to control.
- Hypothyroidism should be treated with very slow escalation of thyroid supplements to avoid exacerbating tachyarrhythmias and heart failure.
- Hyperthyroidism and heart failure create a dangerous combination that merits very close supervision, often hospitalization, during titration of antithyroid medications, during which the decompensation of heart failure may occur precipitously and fatally.
- Patients with pheochromocytoma often have postural hypotension.
- In addition to alpha-adrenergic receptor antagonists, definitive therapy requires surgical extirpation.
- Very high renin states, such as those caused by renal artery stenosis, can lead to modest depression in ejection fraction with little or no ventricular dilation and markedly labile symptoms with flash pulmonary edema, related to sudden shifts in vascular tone and intravascular volume.
7.1 Management of Anthracycline Cardiotoxicity¶
- Therapy for reduced ejection fraction due to anthracycline therapy includes beta-adrenergic receptor blockade and inhibition of the renin-angiotensin system.
- There is conflicting data on whether these agents decrease toxicity when given in parallel with chemotherapy.
- The use of dexrazoxane, an intracellular iron chelating agent, can prevent anthracycline cardiomyopathy.
- There is no consensus on when it should be used owing to concerns that it might attenuate the efficacy of cancer therapies.
7.2 Management of Peripartum Cardiomyopathy¶
- Initial treatment for PPCM includes loop diuretics as needed to restore normal volume status.
- Prior to delivery, close collaboration with the maternal-fetal medicine team is necessary to adjust therapies to stabilize the gravid mother while protecting the fetus.
- Digoxin and beta blockers can be used if needed for arrhythmias.
- Hydralazine/nitrate combinations can be used for hypertension.
- Renin-angiotensin system inhibitors should not be given due to adverse fetal effects.
- Hemodynamic instability may require ongoing hemodynamic monitoring, and plans should be in place for emergency delivery if necessary.
- When the mother is hemodynamically stable in the postpartum period, metoprolol tartrate, enalapril, and spironolactone have been shown to be compatible with breastfeeding.
- PPCM with LVEF <0.35 or marked dilation carries increased incidence of left ventricular thrombus and embolic risk, so anticoagulation is usually prescribed for the first 6 weeks once obstetric bleeding has resolved.
- Breastfeeding was once prohibited but now is generally encouraged in patients in whom fluid balance can be maintained through the high oral fluid intake required.
- For patients who are not breastfeeding, there is an ongoing large, randomized trial to determine the impact of bromocriptine on PPCM outcomes.
7.3 Management of Takotsubo Syndrome¶
- No therapies have been proven beneficial.
- Reasonable strategies include nitrates for pulmonary edema.
- Combined alpha and beta blockers rather than selective beta blockade if hemodynamically stable.
- Magnesium for arrhythmias related to QT prolongation.
- An intra-aortic balloon pump is occasionally employed to improve critically low cardiac output, but only if there is no left ventricular outflow tract obstruction.
7.4 Management of Hemochromatosis¶
- If diagnosed early, hemochromatosis can often be managed by repeated phlebotomy to remove iron.
- For more severe iron overload, iron chelation therapy with desferrioxamine (deferoxamine) or deferasirox can help to improve cardiac function if myocyte loss and replacement fibrosis are not too severe.
7.5 Management of Pheochromocytoma¶
- Patients with pheochromocytoma often have postural hypotension.
- In addition to alpha-adrenergic receptor antagonists, definitive therapy requires surgical extirpation.
8. PROGNOSIS & COMPLICATIONS¶
- Almost a third of patients with recent-onset cardiomyopathy in the absence of coronary artery disease demonstrate substantial spontaneous recovery to normal ejection fraction.
- Partial recovery to left ventricular ejection fraction (LVEF) >0.40 is common in chronic DCM during recommended therapy with neurohormonal modulation, cardiac resynchronization therapy for left bundle branch block, and diuretics as needed to maintain fluid balance.
- Improvement of LVEF to ≥0.50 occurs in 50–80% of PPCM, often within 6 months, when other cardiac diagnoses have been carefully excluded.
- Recovery is less likely with LVEF 6 weeks after delivery.
- Patients with LVEF <0.35 have a higher risk of life-threatening arrhythmias during initial presentation and early after discharge, for which consideration of wearable defibrillators is reasonable.
- One-year mortality rates after PPCM have ranged in the United States from 4% in one study to 11% in a population of black women, and have been reported as up to twofold higher in Africa.
- The long-term prognosis is generally good for Takotsubo syndrome, with the lowest mortality associated with episodes triggered by emotional rather than physical triggers.
- In-hospital complications and mortality are similar to those with acute myocardial infarction for Takotsubo syndrome.
- Recurrence occurs in 10% of patients at an estimated rate of 2%/year for Takotsubo syndrome.
- Trastuzumab cardiomyopathy may persist in about a third of affected patients and can progress to clinical heart failure and death.
- Once thought to have an inexorable downward course, many patients with symptomatic heart failure can improve to near-normal function with careful management, including prevention of 'second-hit' insults and such as atrial fibrillation or hypertension.
- The course differs for some children treated with these agents before puberty, in whom inadequate growth of the heart may lead to refractory heart failure as they reach their twenties.
8.1 PPCM Prognostic Factors¶
- Improvement of LVEF to ≥0.50 occurs in 50–80% of PPCM, often within 6 months.
- Recovery is less likely with LVEF 6 weeks after delivery.
- Patients with LVEF <0.35 have a higher risk of life-threatening arrhythmias during initial presentation and early after discharge.
- Consideration of wearable defibrillators is reasonable for patients with LVEF <0.35.
- One-year mortality rates after PPCM have ranged in the United States from 4% to 11%.
- Mortality rates have been reported as up to twofold higher in Africa.
8.2 Takotsubo Prognosis¶
- The long-term prognosis is generally good.
- The lowest mortality associated with episodes triggered by emotional rather than physical triggers.
- In-hospital complications and mortality are similar to those with acute myocardial infarction.
- Recurrence occurs in 10% of patients at an estimated rate of 2%/year.
9. SPECIAL CONSIDERATIONS¶
- Pregnancy represents another environmental trigger for accelerated phenotypic expression of genetic cardiomyopathy.
- Genetic testing should be considered as the results may impact the mother, in whom positive genetic testing predicts less recovery, and also other family members, too.
- Breastfeeding was once prohibited but now is generally encouraged in patients in whom fluid balance can be maintained through the high oral fluid intake required.
- For patients who are not breastfeeding, there is an ongoing large, randomized trial to determine the impact of bromocriptine on PPCM outcomes.
- The course differs for some children treated with these agents before puberty, in whom inadequate growth of the heart may lead to refractory heart failure as they reach their twenties.
- Nutritional deficiencies can occasionally cause DCM but are not commonly implicated in developed countries.
- Beriberi heart disease due to thiamine deficiency can result from poor nutrition in undernourished populations and in patients deriving most of their calories from alcohol and has been reported in teenagers subsisting only on highly processed foods.
- Abnormalities in carnitine metabolism can cause dilated or restrictive cardiomyopathies, usually in children.
- Deficiency of trace elements such as selenium can cause cardiomyopathy (Keshan's disease).
- Calcium is essential for excitation-contraction coupling.
- Chronic deficiencies of calcium, such as can occur with hypoparathyroidism (particularly postsurgical) or intestinal dysfunction (from diarrheal syndromes and following extensive resection), can cause severe chronic heart failure that responds over days or weeks to vigorous calcium repletion.
- Phosphate is a component of high-energy compounds needed for efficient energy transfer and multiple signaling pathways.
- Hypophosphatemia can develop during starvation and early refeeding following a prolonged fast and occasionally during hyperalimentation.
- Vaccines have occasionally been implicated in myocarditis, particularly after the smallpox vaccine in military populations and more recently with COVID-19 vaccines.
- The risk for men under 40 increases after repeat COVID-19 vaccines, for which the benefit/risk for individuals should be considered.
- Male adults under 40 are at highest risk of myocarditis from the COVID-19 vaccines, as they are for primary infectious myocarditis after COVID-19 and other viruses.
9.1 Pregnancy and Breastfeeding¶
- Pregnancy represents another environmental trigger for accelerated phenotypic expression of genetic cardiomyopathy.
- Genetic testing should be considered as the results may impact the mother, in whom positive genetic testing predicts less recovery, and also other family members, too.
- Breastfeeding was once prohibited but now is generally encouraged in patients in whom fluid balance can be maintained through the high oral fluid intake required.
- For patients who are not breastfeeding, there is an ongoing large, randomized trial to determine the impact of bromocriptine on PPCM outcomes.
9.2 Pediatric Considerations¶
- The course differs for some children treated with these agents before puberty, in whom inadequate growth of the heart may lead to refractory heart failure as they reach their twenties.
- Abnormalities in carnitine metabolism can cause dilated or restrictive cardiomyopathies, usually in children.
- Deficiency of trace elements such as selenium can cause cardiomyopathy (Keshan's disease).
9.3 Nutritional Deficiencies¶
- Nutritional deficiencies can occasionally cause DCM but are not commonly implicated in developed countries.
- Beriberi heart disease due to thiamine deficiency can result from poor nutrition in undernourished populations and in patients deriving most of their calories from alcohol and has been reported in teenagers subsisting only on highly processed foods.
- Calcium is essential for excitation-contraction coupling.
- Chronic deficiencies of calcium, such as can occur with hypoparathyroidism (particularly postsurgical) or intestinal dysfunction (from diarrheal syndromes and following extensive resection), can cause severe chronic heart failure that responds over days or weeks to vigorous calcium repletion.
- Phosphate is a component of high-energy compounds needed for efficient energy transfer and multiple signaling pathways.
- Hypophosphatemia can develop during starvation and early refeeding following a prolonged fast and occasionally during hyperalimentation.
10. KEY PEARLS & CLINICAL TRAPS¶
- Alcoholic cardiomyopathy remains a diagnosis of exclusion.
- Mendelian randomization studies have not identified a link between genetically predicated alcohol consumption and heart failure, suggesting that the population attributable risk of alcohol to the overall heart failure epidemic is modest.
- Mutations in TTN and other DCM disease genes can be identified in ~10% of patients with presumed alcohol cardiomyopathy.
- PPCM recovery to LVEF ≥0.50 occurs in 50–80% of cases within 6 months; recovery is less likely with LVEF 6 weeks after delivery.
- Takotsubo syndrome typically resolves within days to weeks; recurrence occurs in 10% of patients at an estimated rate of 2%/year.
- Checkpoint inhibitor myocarditis requires immediate high-dose glucocorticoids; outcomes are improving with earlier recognition and therapy.
- Hemochromatosis diagnosis is made principally by MRI iron quantitation; phlebotomy is the management for early disease to remove iron.
- Trastuzumab cardiomyopathy may persist in about a third of affected patients and can progress to clinical heart failure and death.
- PPCM anticoagulation is usually prescribed for the first 6 weeks postpartum if LVEF <0.35 or marked dilation is present due to thrombus risk.
- TTN truncating mutations are found in ~15% of PPCM cases and are associated with lower rates of recovered systolic function.
- Vaccine-induced myocarditis risk after COVID-19 vaccines is estimated at 1/100,000 doses, increasing to 2–3/100,000 for recipients age 18–39 years.
- Male adults under 40 are at highest risk of myocarditis from the COVID-19 vaccines, as they are for primary infectious myocarditis after COVID-19 and other viruses.
- The most dramatic form of noninfectious inflammatory myocarditis is that seen with combined immune checkpoint inhibitors.
- Cardiotoxicity has been reported with multiple environmental and pharmacologic agents.
- Chemotherapy agents are the most common drugs implicated in toxic cardiomyopathy.
- Vascular endothelial growth factor (VEGF), produced endogenously or by tumors, enhances angiogenesis by activating the VEGF signaling pathways.
- Monoclonal antibodies and many small-molecule tyrosine kinase inhibitors that affect VEGF are in use for different malignancies.
- Blood pressures increase in most patients during therapy, attributed to an imbalance between endogenous vasodilators and vasoconstrictors and alteration of glomerular function.
- Hypertension and proteinuria can develop with these agents, similar to preeclampsia, and presentation is associated with increased risk of future cardiac disease.
- Recognition of cardiotoxicity during therapy with these agents is complicated because they occasionally cause peripheral fluid accumulation (ankle edema, periorbital swelling, pleural effusions) due to local factors rather than elevated central venous pressures.
- Therapeutic approaches include management of associated hypertension, withdrawal of the tyrosine kinase inhibitor (when possible), and conventional treatment for heart failure.
- Newer tyrosine kinase inhibitors effective against multiple kinases may have more complex off-target effects.
- This includes the Bruton tyrosine kinase inhibitors (e.g., ibrutinib), which are used as primary therapy for lymphoid malignancies, with predominant cardiovascular risks of atrial and ventricular arrhythmias in addition to heart failure.
- Proteasome inhibitors used to treat multiple myeloma are associated with an increased risk of hypertension, ischemic events, thromboembolism, and heart failure.
- The more potent agent, carfilzomib, appears more cardiotoxic than bortezomib.
- Other treatments for myeloma include immunomodulatory drugs including lenalidomide and thalidomide, which may cause heart failure in addition to risks of venous thromboembolism.
- Mitogen-activated extracellular signal regulated kinase (MEK) inhibitors used for metastatic melanoma may cause brain hypertension and cardiomyopathy, especially when co-administered with rapidly accelerated fibrosarcoma (RAF) inhibitors.
- Diabetes mellitus is a typical factor in heart failure with 'preserved' ejection fraction, along with hypertension, advanced age, and female gender.
- The existence of a cardiomyopathy due to obesity is generally accepted, but the overlap is not well defined with the syndrome of heart failure with preserved ejection fraction (HFpEF).
- In the absence of another obvious cause of cardiomyopathy in an obese patient with systolic dysfunction without marked ventricular dilation, effective weight reduction is often associated with major improvement in ejection fraction and clinical function.
- Improvement in cardiac function has been described after successful bariatric surgery, although all major surgical therapy poses increased risk for patients with heart failure.
- Postoperative malabsorption and nutritional deficiencies, such as calcium and phosphate deficiencies, may be particularly deleterious for patients with cardiomyopathy.
- Hyperthyroidism should always be considered with new-onset atrial fibrillation or ventricular tachycardia or atrial fibrillation in which the rapid ventricular response is difficult to control.
- Hypothyroidism should be treated with very slow escalation of thyroid supplements to avoid exacerbating tachyarrhythmias and heart failure.
- Hyperthyroidism and heart failure create a dangerous combination that merits very close supervision, often hospitalization, during titration of antithyroid medications, during which the decompensation of heart failure may occur precipitously and fatally.
- Patients with pheochromocytoma often have postural hypotension.
- In addition to alpha-adrenergic receptor antagonists, definitive therapy requires surgical extirpation.
- Very high renin states, such as those caused by renal artery stenosis, can lead to modest depression in ejection fraction with little or no ventricular dilation and markedly labile symptoms with flash pulmonary edema, related to sudden shifts in vascular tone and intravascular volume.
10.1 Diagnostic Pitfalls¶
- Alcoholic cardiomyopathy remains a diagnosis of exclusion.
- Mendelian randomization studies have not identified a link between genetically predicated alcohol consumption and heart failure.
- Mutations in TTN and other DCM disease genes can be identified in ~10% of patients with presumed alcohol cardiomyopathy.
- Recognition of cardiotoxicity during therapy with these agents is complicated because they occasionally cause peripheral fluid accumulation (ankle edema, periorbital swelling, pleural effusions) due to local factors rather than elevated central venous pressures.
- The existence of a cardiomyopathy due to obesity is generally accepted, but the overlap is not well defined with the syndrome of heart failure with preserved ejection fraction (HFpEF).
10.2 Treatment Traps¶
- There is no consensus on when dexrazoxane should be used owing to concerns that it might attenuate the efficacy of cancer therapies.
- Renin-angiotensin system inhibitors should not be given in PPCM due to adverse fetal effects.
- Breastfeeding was once prohibited but now is generally encouraged in patients in whom fluid balance can be maintained through the high oral fluid intake required.
- For patients who are not breastfeeding, there is an ongoing large, randomized trial to determine the impact of bromocriptine on PPCM outcomes.
- An intra-aortic balloon pump is occasionally employed to improve critically low cardiac output, but only if there is no left ventricular outflow tract obstruction.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
Caption: FIGURE 269-1 Hemochromatosis. Microscopic image of an endomyocardial biopsy showing extensive iron deposition within the cardiac myocytes with the Prussian blue stain (400× original magnification). (Image courtesy of Robert Padera, MD, PhD, Department of Pathology, Brigham and Women’s Hospital, Boston.) mitochondrial function. A diagnosis of systemic iron overload is made from measurement of serum iron and transferrin saturation, with a threshold of >60% for men and >45–50% for women. MRI is used to in quantitate iron stores in the liver and heart. While endomyocardial biopsy tissue can be stained for iron (see Chap. 270 and Fig. 269-1), — Hemochromatosis. Microscopic image of an endomyocardial biopsy showing extensive iron deposition within the cardiac myocytes with the Prussian blue stain (400× original magnification).
Figure 2¶
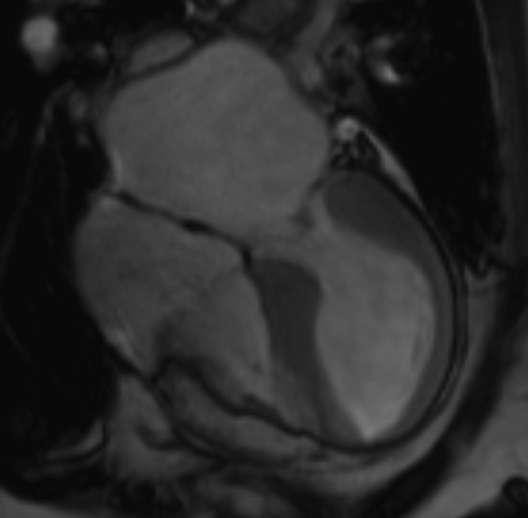
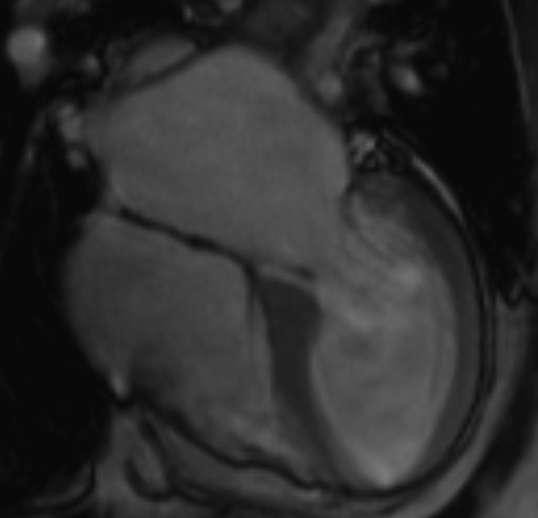
Caption: FIGURE 269-1 Hemochromatosis. Microscopic image of an endomyocardial biopsy showing extensive iron deposition within the cardiac myocytes with the Prussian blue stain (400× original magnification). (Image courtesy of Robert Padera, MD, PhD, Department of Pathology, Brigham and Women’s Hospital, Boston.) mitochondrial function. A diagnosis of systemic iron overload is made from measurement of serum iron and transferrin saturation, with a threshold of >60% for men and >45–50% for women. MRI is used to in quantitate iron stores in the liver and heart. While endomyocardial biopsy tissue can be stained for iron (see Chap. 270 and Fig. 269-1), — Takotsubo cardiomyopathy. Four-chamber view of cardiac magnetic resonance imaging demonstrating a mildly dilated left ventricle in diastole with diffuse hypokinesis of the mid and apical segments and relative sparing of the basal segment wall motion at end systole.
Figure 3¶
Caption: FIGURE 269-1 Hemochromatosis. Microscopic image of an endomyocardial biopsy showing extensive iron deposition within the cardiac myocytes with the Prussian blue stain (400× original magnification). (Image courtesy of Robert Padera, MD, PhD, Department of Pathology, Brigham and Women’s Hospital, Boston.) mitochondrial function. A diagnosis of systemic iron overload is made from measurement of serum iron and transferrin saturation, with a threshold of >60% for men and >45–50% for women. MRI is used to in quantitate iron stores in the liver and heart. While endomyocardial biopsy tissue can be stained for iron (see Chap. 270 and Fig. 269-1), — Takotsubo cardiomyopathy. Electrocardiogram showing ST-segment elevation and T-wave inversion mimicking acute myocardial infarction in the setting of stress-induced cardiomyopathy.
Figure 4¶
Caption: Dilated Cardiomyopathy Phenotype. Schematic diagram illustrating the characteristic phenotype of decreased left ventricular systolic function with increased left ventricular dimensions and secondary mitral regurgitation.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.