Renovascular Disease¶
Chapter 289 | Part 6: Disorders of the Cardiovascular System · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Critical renal artery stenosis is defined as >70–80% luminal obstruction, activating the renin-angiotensin system and sympathetic pathways.
- Fibromuscular dysplasia (FMD) affects younger women (age 15–50) and does not typically threaten kidney function unless total occlusion occurs.
- Atherosclerotic renal artery stenosis (ARAS) prevalence is 6.8% in community samples >65 years and increases with age and comorbidities.
- Revascularization restores renal blood flow but recovery of renal function is limited to ~25% of cases; recovery is absent in 50%.
- Atheroembolic renal disease presents with livedo reticularis, toe gangrene, eosinophilia (60–80%), and hypocomplementemia (15%).
- Malignant hypertension is characterized by fibrinoid necrosis and 'onionskin' lesions in interlobular arteries, with mortality >50% over 6–12 months if untreated.
- Revascularization is indicated for rapidly progressive clinical syndromes, failing medical therapy, or developing additional complications.
- Medical therapy for ARAS includes RAAS blockade, goal blood pressure attainment, tobacco cessation, statins, and aspirin.
- Magnetic resonance angiography (MRA) is contraindicated in GFR <30 mL/min/1.73 m2 due to gadolinium toxicity risk.
- Duplex ultrasonography is the preferred initial noninvasive test, showing renal arteries and measuring flow velocity to assess stenosis severity.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Mechanisms of Vascular Injury and Hypertension
- 1.2 Pathophysiology of Renovascular Hypertension
- 2. EPIDEMIOLOGY
- 2.1 Demographic Distribution
- 2.2 Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Atherosclerotic Renal Artery Stenosis (ARAS)
- 3.2 Fibromuscular Dysplasia (FMD)
- 3.3 Atheroembolic Renal Disease
- 3.4 Thromboembolic Renal Disease
- 3.5 Microvascular Injury and Malignant Hypertension
- 4. CLINICAL FEATURES
- 4.1 Symptoms and Signs of ARAS
- 4.2 Symptoms and Signs of FMD
- 4.3 Symptoms and Signs of Atheroembolic Disease
- 4.4 Symptoms and Signs of Thromboembolic Disease
- 4.5 Symptoms and Signs of Malignant Hypertension
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 ARAS vs FMD
- 5.2 Renovascular vs Essential Hypertension
- 5.3 Atheroembolic vs Thromboembolic
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Perfusion Studies
- 6.2 Vascular Studies
- 6.3 Diagnostic Criteria and Thresholds
- 7. MANAGEMENT & TREATMENT
- 7.1 Medical Therapy
- 7.2 Revascularization
- 7.3 Atheroembolic Renal Disease Management
- 7.4 Thromboembolic Renal Disease Management
- 7.5 Malignant Hypertension Management
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 ARAS Prognosis
- 8.2 Atheroembolic Disease Prognosis
- 8.3 Malignant Hypertension Prognosis
- 9. SPECIAL CONSIDERATIONS
- 9.1 Elderly Patients
- 9.2 Renal Impairment
- 9.3 Comorbidities
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Clues
- 10.2 Exclusion Criteria
- 10.3 Treatment Pearls
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Examples of micro-CT images from vessels defined by radiopaque casts capillary network... |
| 2 | 🖼 Figure | A |
| 3 | 🖼 Figure | A |
| 4 | 🖼 Figure | Figure / Illustration |
1. DEFINITION & OVERVIEW¶
Renovascular disease encompasses disorders of the renal vasculature that threaten blood supply to the kidney. The renal vasculature is unusually complex with high arteriolar flow rate to the cortex in excess of metabolic requirements. After delivering blood to cortical glomeruli, the postglomerular circulation supplies deeper medullary segments that support energy-dependent solute transport. Vascular disorders threatening the blood supply include large-vessel atherosclerosis, fibromuscular diseases, and embolic disorders. Microvascular injury is described in other chapters.
1.1 Mechanisms of Vascular Injury and Hypertension¶
Activation of the renin-angiotensin system is a key step in developing renovascular hypertension, but it is transient. Levels of renin activity are subject to timing, drug effects, and sodium intake. Large-vessel renal artery occlusive disease can result from extrinsic compression, intimal dissection, aortic stent graft placement, fibromuscular dysplasia (FMD), or most commonly, atherosclerotic disease. Any disorder reducing perfusion pressure activates mechanisms restoring renal pressures at the expense of systemic hypertension.
1.2 Pathophysiology of Renovascular Hypertension¶
Critical levels of stenosis (usually >70–80% luminal obstruction) lead to reduced perfusion pressure, activating the renin-angiotensin system, reducing sodium excretion, and activating sympathetic adrenergic pathways. These events lead to systemic hypertension characterized by angiotensin dependence in early stages, widely varying pressures, loss of circadian blood pressure rhythms, and accelerated target organ injury including left ventricular hypertrophy and renal fibrosis. Renovascular hypertension can be treated with agents that block the renin-angiotensin system and other drugs that modify pressor pathways. It can also be treated with restoration of renal blood flow by either endovascular or surgical revascularization. Most patients require continued antihypertensive drug therapy due to preexisting hypertension and because revascularization alone rarely lowers BP to normal.
2. EPIDEMIOLOGY¶
Renovascular disease prevalence varies by etiology and demographic factors. Atherosclerotic renal artery stenosis (ARAS) is common in the general population (6.8% of a community-based sample above age 65). The prevalence increases with age and for patients with other vascular conditions such as coronary artery disease (18–23%) and/or peripheral aortic or lower extremity disease (>30%). Fibromuscular dysplasia (FMD) is reported in 3–5% of normal subjects presenting as potential kidney donors without hypertension. It may present clinically with hypertension in younger individuals (between age 15 and 50), most often women. Atheroembolic renal disease is suspected in >3% of elderly subjects with end-stage renal disease (ESRD) and is likely underdiagnosed. It is more frequent in males with a history of diabetes, hypertension, and cardiac disease.
2.1 Demographic Distribution¶
- ARAS: Common in general population, prevalence increases with age.
- FMD: Reported in 3–5% of normal subjects, presents in younger individuals (age 15–50), most often women.
- Atheroembolic Disease: Suspected in >3% of elderly subjects with ESRD, more frequent in males with diabetes, hypertension, and cardiac disease.
2.2 Risk Factors¶
- Modifiable: Tobacco use, hypertension, diabetes, dyslipidemia.
- Non-modifiable: Age, race (implied by general population prevalence), genetic predisposition to FMD.
- Comorbidities: Coronary artery disease, peripheral aortic or lower extremity disease.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Large-vessel renal artery occlusive disease can result from multiple conditions including extrinsic compression of the vessel, intimal dissection, aortic stent graft placement, fibromuscular dysplasia (FMD), or most commonly, atherosclerotic disease. Microvascular injury, including inflammatory and primary hematologic disorders, is described in other chapters. The glomerular capillary endothelium shares susceptibility to oxidative stress, pressure injury, and inflammation with other vascular territories. Endothelial injury can be manifest by urinary albumin excretion (UAE), which is predictive of systemic atherosclerotic disease events. Increased UAE may develop years before cardiovascular events. UAE and the risk of cardiovascular events are both reduced with pharmacologic therapy such as antihypertensive drugs and statins.
3.1 Atherosclerotic Renal Artery Stenosis (ARAS)¶
ARAS is common in the general population (6.8% of a community-based sample above age 65). The prevalence increases with age and for patients with other vascular conditions such as coronary artery disease (18–23%) and/or peripheral aortic or lower extremity disease (>30%). ARAS develops in patients with other risk factors for atherosclerosis and is commonly superimposed upon preexisting small-vessel disease in the kidney resulting from hypertension, aging, and diabetes. Nearly 85% of patients considered for renal revascularization have stage 3–5 chronic kidney disease (CKD) with estimated GFR <60 mL/min per 1.73 m2.
3.2 Fibromuscular Dysplasia (FMD)¶
FMD is reported in 3–5% of normal subjects presenting as potential kidney donors without hypertension. It may present clinically with hypertension in younger individuals (between age 15 and 50), most often women. FMD does not often threaten kidney function, but sometimes produces total occlusion and can be associated with renal artery aneurysms. Patients with FMD are commonly younger females with otherwise normal vessels and a long life expectancy. These patients often respond well to percutaneous and/or renal artery angioplasty.
3.3 Atheroembolic Renal Disease¶
Emboli to the kidneys arise most frequently as a result of cholesterol crystals breaking free of atherosclerotic vascular plaque and lodging in downstream microvessels. Most clinical atheroembolic events follow angiography, vascular surgery, anticoagulation with heparin, thrombolytic therapy, or trauma. Atheroemboli in the kidney are strongly associated with aortic aneurysmal disease and renal artery stenosis. Silent cholesterol emboli are frequently present before any further manipulation is performed. Biopsies obtained from patients undergoing surgical revascularization indicate that silent cholesterol emboli are frequently present before any further manipulation is performed.
3.4 Thromboembolic Renal Disease¶
Thrombotic occlusion of renal vessels or branch arteries can lead to declining renal function and hypertension. It is difficult to diagnose. Thrombosis can develop as a result of local vessel abnormalities, such as local dissection, trauma, inflammatory vasculitis, or systemic infections, such as COVID-19. Local microdissections sometimes lead to patchy, transient areas of infarctions labeled 'segmental arteriolar mediolysis.' It can also derive from distant embolic events, e.g., the left atrium in patients with atrial fibrillation or from fat emboli originating from traumatized tissue, most commonly large bone fractures. Cardiac sources include vegetations from subacute bacterial endocarditis. Systemic emboli to the kidneys may also arise from the venous circulation if right-to-left shunting occurs, e.g., through a patent foramen ovale.
3.5 Microvascular Injury and Malignant Hypertension¶
Microvascular injury associated with hypertension includes arteriolonephrosclerosis. 'Malignant' hypertension is characterized by rapidly progressive BP elevations with target organ injury including retinal hemorrhages, encephalopathy, and declining kidney function. If untreated, patients with target organ injury including papilledema and declining kidney function suffered mortality rates in excess of 50% over 6–12 months, hence the designation 'malignant.' Postmortem studies identified vascular lesions designated 'fibrinoid necrosis,' with breakdown of the vessel wall, deposition of eosinophilic material including fibrin, and a perivascular cellular infiltrate. A separate lesion was identified in the larger interlobular arteries in many patients with hyperplastic proliferation of the vascular wall cellular elements, deposition of collagen, and separation of layers, designated the 'onionskin' lesion.
4. CLINICAL FEATURES¶
Renovascular disease presents with hypertension, which can be refractory to effective therapy. Clinical manifestations vary depending on the rapidity of onset and extent of occlusion. Acute arterial thrombosis may produce flank pain, fever, leukocytosis, nausea, and vomiting. If kidney infarction results, enzymes such as lactate dehydrogenase (LDH) rise transiently to extreme levels. If both kidneys are affected, renal function will decline precipitously with a drop in urine output. If a single kidney is involved, renal functional changes may be minor. Hypertension related to sudden release of renin from ischemic tissue can develop rapidly, as long as some viable tissue in the 'peri-infarct' border zone remains. If the infarct zone demarcates precisely, the rise in BP and renin activity may resolve.
4.1 Symptoms and Signs of ARAS¶
- Hypertension: Often refractory to effective therapy.
- Flank pain: May occur with acute thrombosis.
- Fever, leukocytosis, nausea, vomiting: Associated with acute arterial thrombosis.
- Target organ injury: Left ventricular hypertrophy, renal fibrosis.
4.2 Symptoms and Signs of FMD¶
- Hypertension: In younger individuals (age 15–50).
- Renal artery aneurysms: Can be associated with FMD.
- Total occlusion: Sometimes produces total occlusion.
- Recovery: Often respond well to percutaneous and/or renal artery angioplasty.
4.3 Symptoms and Signs of Atheroembolic Disease¶
- Cutaneous manifestations: Livedo reticularis and localized toe gangrene may be more common.
- Systemic manifestations: Fever, abdominal pain, and weight loss are present in less than half of patients.
- Worsening hypertension and deteriorating kidney function: Common, sometimes reaching a malignant phase.
- Laboratory findings: Rising creatinine, transient eosinophilia (60–80%), elevated sedimentation rate, and hypocomplementemia (15%).
4.4 Symptoms and Signs of Thromboembolic Disease¶
- Acute arterial thrombosis: Flank pain, fever, leukocytosis, nausea, vomiting.
- Kidney infarction: LDH rise transiently to extreme levels.
- Bilateral involvement: Renal function declines precipitously with drop in urine output.
- Unilateral involvement: Renal functional changes may be minor.
4.5 Symptoms and Signs of Malignant Hypertension¶
- Target organ injury: Retinal hemorrhages, encephalopathy, declining kidney function.
- Vascular lesions: Fibrinoid necrosis, 'onionskin' lesion in interlobular arteries.
- Mortality: Exceeds 50% over 6–12 months if untreated.
5. DIFFERENTIAL DIAGNOSIS¶
Differential diagnosis includes essential hypertension, atherosclerotic renal artery stenosis (ARAS), fibromuscular dysplasia (FMD), atheroembolic renal disease, thromboembolic renal disease, and arteriolonephrosclerosis. Distinguishing features include age, presence of atherosclerosis risk factors, cutaneous findings (livedo reticularis), and response to medical therapy.
5.1 ARAS vs FMD¶
- ARAS: Common in older individuals with preexisting atherosclerotic risk factors.
- FMD: Common in younger females (age 15–50) with otherwise normal vessels.
- Imaging: FMD often shows characteristic beading or string-of-beads appearance on angiography (implied by FMD diagnosis).
5.2 Renovascular vs Essential Hypertension¶
- Renovascular: Angiotensin dependence in early stages, widely varying pressures, loss of circadian BP rhythms.
- Essential: Stable BP control with optimal medical therapy.
- Revascularization benefit: Small mortality benefit for stented patients without proteinuria in ARAS.
5.3 Atheroembolic vs Thromboembolic¶
- Atheroembolic: Cholesterol crystals, livedo reticularis, eosinophilia, hypocomplementemia.
- Thromboembolic: Local dissection, trauma, systemic infections, atrial fibrillation, fat emboli.
6. INVESTIGATIONS & DIAGNOSIS¶
Diagnostic approaches to renovascular disease necessarily include evaluation of the kidney vasculature and depend on the specific clinical questions to be addressed. Noninvasive characterization of the renal vasculature may be achieved by several techniques. Although activation of the renin-angiotensin system is a key step in developing renovascular hypertension, it is transient. Levels of renin activity are therefore subject to timing, the effects of drugs, and sodium intake, and do not reliably predict the response to vascular therapy. Peak systolic renal artery velocities by Doppler ultrasound >200 cm/s generally predict lesions with more than >60% vessel lumen occlusion, although some treatment trials have required velocity >300 cm/s to avoid false positives. The renal resistive index has predictive value regarding the viability of the kidney. It remains operator- and institution-dependent, however.
6.1 Perfusion Studies¶
- Captopril renography with technetium-99m mertiatide (99mTc MAG3): Captopril-mediated fall in filtration pressure amplifies differences in renal perfusion.
- Utility: Normal study excludes renovascular hypertension.
- Limitations: Multiple limitations in patients with advanced atherosclerosis or creatinine >2.0 mg/dL (177 μmol/L).
Table 1 — Table 289-1 Summary of Imaging Modalities for Evaluating the Kidney Vasculature¶
| Modality | Description | Advantages | Limitations |
|---|---|---|---|
| Captopril renography with technetium-99m mertiatide (99mTc MAG3) | Captopril-mediated fall in filtration pressure amplifies differences in renal perfusion | Normal study excludes renovascular hypertension | Multiple limitations in patients with advanced atherosclerosis or creatinine >2.0 mg/dL (177 μmol/L) |
| Duplex ultrasonography | Shows the renal arteries and measures flow velocity as a means for follow-up studies | Inexpensive; widely available, suitable for follow-up studies | Heavily dependent on operator's experience; less than invasive angiography for the diagnosis of fibromuscular dysplasia and abnormalities in accessory renal arteries |
| Computed tomographic angiography | Shows the renal arteries and perirenal aorta | Provides excellent images; stents do not cause artifacts | Expensive, moderate volume of contrast required |
| Magnetic resonance angiography | Shows the renal arteries and perirenal aorta | Not nephrotoxic, but concerns for gadolinium toxicity exclude use in GFR <30 mL/min/1.73 m2; provides excellent images | Expensive; gadolinium excluded in renal failure, unable to visualize stented vessels |
| Intraarterial angiography | Shows location and severity of vascular lesion | Considered 'gold standard' for diagnosis of large-vessel disease, usually performed simultaneous with planned intervention | Expensive, associated hazard of atheroemboli, contrast toxicity, procedure-related complications, e.g., dissection |
6.2 Vascular Studies¶
- Duplex ultrasonography: Shows the renal arteries and measures flow velocity as a means for follow-up studies of assessing the severity of stenosis.
- Computed tomographic angiography: Shows the renal arteries and perirenal aorta. Provides excellent images; stents do not cause artifacts.
- Magnetic resonance angiography: Shows the renal arteries and perirenal aorta. Not nephrotoxic, but concerns for gadolinium toxicity exclude use in GFR <30 mL/min/1.73 m2; provides excellent images.
- Intraarterial angiography: Shows location and severity of vascular lesion. Considered 'gold standard' for diagnosis of large-vessel disease, usually performed simultaneous with planned intervention.
6.3 Diagnostic Criteria and Thresholds¶
- Critical stenosis: Usually >70–80% luminal obstruction.
- Doppler velocity: >200 cm/s generally predict lesions with more than >60% vessel lumen occlusion.
- Doppler velocity threshold for trials: >300 cm/s to avoid false positives.
- Captopril renography: Normal study excludes renovascular hypertension.
- GFR threshold for MRA: <30 mL/min/1.73 m2.
7. MANAGEMENT & TREATMENT¶
Renal revascularization should be considered for patients with rapidly progressive clinical syndromes, failing medical therapy, and/or developing additional complications. Techniques of renal revascularization are improving. With experienced operators, major complications occur in <5% of cases, including renal artery dissection, capsular perforation, hemorrhage, and occasional atheroembolic disease. Although not common, atheroembolic disease can be catastrophic and accelerate both hypertension and kidney failure, precisely the events that revascularization is intended to prevent. Although renal blood flow usually can be restored by endovascular stenting, recovery of renal function is limited to ~25% of cases, with no change in 50% and some deterioration evident in others. Patients with rapid loss of kidney function, sometimes associated with antihypertensive drug therapy, or vascular disease affecting the entire functioning kidney mass allude to loss of BP control. Renal revascularization should be considered for patients with rapidly progressive clinical syndromes, failing medical therapy, and/or developing additional complications.
7.1 Medical Therapy¶
Medical therapy should include blockade of the renin-angiotensin system, attainment of goal BPs, blockade of tobacco, statins, and aspirin. Follow-up requires surveillance for progressive occlusion manifest by worsening renal function with loss of BP control. Medical therapy with follow-up for disease progression is equally effective over periods of 3–5 years in patients with moderate stenosis where multiple prospective randomized controlled trials have failed to identify compelling additional benefits for intervention.
Table 2 — Table 289-2 Clinical Factors That Determine the Role of Revascularization in Addition to Medical Therapy for Renal Artery Stenosis¶
| Category | Factors |
|---|---|
| Factors Favoring Medical Therapy with Revascularization for Renal Artery Stenosis | • Progressive decline in GFR during treatment of systemic hypertension • Failure to achieve adequate blood pressure control with optimal medical therapy (medical failure) • Rapid or recurrent decline in the GFR in association with a reduction in systemic pressure • Decline in the GFR during therapy with ACE inhibitors or ARBs • Recurrent congestive heart failure in a patient in whom left ventricular dysfunction does not fully explain the cause |
| Factors Favoring Medical Therapy and Surveillance of Renal Artery Disease | • Controlled blood pressure with stable renal function (e.g., stable renal insufficiency) and is often overlooked, especially in elderly patients. • Stable renal artery stenosis without progression on surveillance studies (e.g., serial duplex ultrasound) • Advanced age and/or limited life expectancy • Extensive comorbidity that make revascularization too risky • High risk for or previous experience with atheroembolic disease • Other concomitant renal parenchymal diseases that cause progressive renal dysfunction (e.g., interstitial nephritis, diabetic nephropathy), particularly with proteinuria |
7.2 Revascularization¶
- Indications: Rapidly progressive clinical syndromes, failing medical therapy, developing additional complications.
- Techniques: Endovascular or surgical revascularization.
- Complications: Renal artery dissection, capsular perforation, hemorrhage, occasional atheroembolic disease.
- Recovery: Renal blood flow usually can be restored by endovascular stenting, recovery of renal function is limited to ~25% of cases, with no change in 50% and some deterioration evident in others.
- Major complications: Occur in <5% of cases with experienced operators.
7.3 Atheroembolic Renal Disease Management¶
- No effective therapy is available for atheroembolic disease once it has developed.
- Withdrawal of anticoagulation is recommended.
- Late recovery of kidney function after supportive measures sometimes occurs, and statin therapy may improve outcome.
- The role of embolic protection devices in the renal circulation during angiography is unclear, but a few prospective trials have failed to demonstrate major benefits.
- The effect of such devices is limited to distal protection during the endovascular procedure, and they offer no protection from embolic debris developing after removal.
7.4 Thromboembolic Renal Disease Management¶
- Options for interventions of newly detected arterial occlusion include surgical reconstruction, anticoagulation, thrombolytic therapy, endovascular procedures, and supportive care, particularly antihypertensive drug therapy.
- Application of these methods depends on the patient's overall condition, the precipitating factors (e.g., local trauma or systemic illness), the magnitude of renal tissue and function at risk, and the likelihood of recurrent events in the future.
- For unilateral disease, for example, arterial dissection with thrombosis and supportive care with anticoagulation may suffice.
- Acute, bilateral occlusion is potentially catastrophic, producing anuric renal failure. Depending on the precipitating event, surgical or thrombolytic therapies can sometimes restore kidney viability if undertaken early in the course of the acute event.
7.5 Malignant Hypertension Management¶
- Treatment: Antihypertensive drug therapy.
- Pathology: Fibrinoid necrosis, 'onionskin' lesion.
- Prognosis: Mortality rate after 1 year exceeds 38%.
- Recovery: Some may eventually recover sufficiently to no longer require dialysis, many do not.
8. PROGNOSIS & COMPLICATIONS¶
Renovascular disease is considered a specifically treatable 'secondary' cause of hypertension. The presence of ARAS is a strong predictor of morbidity- and mortality-related cardiovascular events, independent of whether renal revascularization is undertaken. Studies of cardiovascular outcomes, including stroke, congestive heart failure, myocardial infarction, and end-stage renal failure, suggest a small mortality benefit for stented patients without proteinuria. Atheroembolic renal disease has an ominous prognosis. Mortality rate after 1 year exceeds 38%, and although some may eventually recover sufficiently to no longer require dialysis, many do not. Malignant hypertension patients suffered mortality rates in excess of 50% over 6–12 months if untreated.
8.1 ARAS Prognosis¶
- Revascularization: Recovery of renal function is limited to ~25% of cases, with no change in 50% and some deterioration evident in others.
- Medical therapy: Equally effective over periods of 3–5 years for moderate stenosis.
- Cardiovascular outcomes: Small mortality benefit for stented patients without proteinuria.
- Predictor: Strong predictor of morbidity- and mortality-related cardiovascular events.
8.2 Atheroembolic Disease Prognosis¶
- Mortality: Exceeds 38% after 1 year.
- Recovery: Some may eventually recover sufficiently to no longer require dialysis, many do not.
- Progression: Progressive renal failure can occur and require dialytic support.
- Onset: Develops after a stuttering onset over many weeks and have an ominous prognosis.
8.3 Malignant Hypertension Prognosis¶
- Mortality: Exceeds 50% over 6–12 months if untreated.
- Target organ injury: Retinal hemorrhages, encephalopathy, declining kidney function.
- Vascular lesions: Fibrinoid necrosis, 'onionskin' lesion.
9. SPECIAL CONSIDERATIONS¶
Special considerations include pregnancy, pediatrics, elderly, renal/hepatic impairment, immunocompromised. The text explicitly mentions advanced age and/or limited life expectancy as factors favoring medical therapy. It also mentions GFR <30 mL/min/1.73 m2 as a contraindication for MRA. It mentions ESRD in the context of atheroembolic disease. It mentions diabetic nephropathy and interstitial nephritis as concomitant renal parenchymal diseases.
9.1 Elderly Patients¶
- Advanced age and/or limited life expectancy favor medical therapy and surveillance.
- Stable renal artery stenosis without progression on surveillance studies (e.g., serial duplex ultrasound).
- Often overlooked, especially in elderly patients.
9.2 Renal Impairment¶
- GFR 2.0 mg/dL (177 μmol/L): Captopril renography has multiple limitations.
- Advanced atherosclerosis: Captopril renography has multiple limitations.
9.3 Comorbidities¶
- Diabetic nephropathy: Concomitant renal parenchymal disease causing progressive renal dysfunction, particularly with proteinuria.
- Interstitial nephritis: Concomitant renal parenchymal disease causing progressive renal dysfunction.
- Coronary artery disease: 18–23% prevalence in ARAS patients.
- Peripheral aortic or lower extremity disease: >30% prevalence in ARAS patients.
10. KEY PEARLS & CLINICAL TRAPS¶
Board-exam favorites, common diagnostic pitfalls, must-not-miss diagnoses, useful mnemonics. The text highlights specific findings and thresholds.
10.1 Diagnostic Clues¶
- Critical stenosis: Usually >70–80% luminal obstruction.
- Doppler velocity: >200 cm/s generally predict lesions with more than >60% vessel lumen occlusion.
- Captopril renography: Normal study excludes renovascular hypertension.
- Atheroembolic disease: Livedo reticularis, localized toe gangrene, eosinophilia (60–80%), hypocomplementemia (15%).
- Malignant hypertension: Fibrinoid necrosis, 'onionskin' lesion.
- FMD: Younger individuals (age 15–50), most often women.
10.2 Exclusion Criteria¶
- Stable renal artery stenosis without progression on surveillance studies.
- Controlled blood pressure with stable renal function.
- Normal captopril renography excludes renovascular hypertension.
- Advanced age and/or limited life expectancy favor medical therapy.
- Extensive comorbidity that make revascularization too risky.
10.3 Treatment Pearls¶
- Revascularization recovery: Limited to ~25% of cases.
- Medical therapy: RAAS blockade, goal BPs, tobacco cessation, statins, aspirin.
- Atheroembolic disease: Withdrawal of anticoagulation recommended.
- MRA: Contraindicated in GFR <30 mL/min/1.73 m2.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 289-1 Examples of micro-CT images from vessels defined by radiopaque casts capillary network supplying the kidney cortex that can either proliferate or succumb Changes in blood supply are followed by tubulointerstitial fibrosis and loss of kidney Angiogenesis in the kidney: A new therapeutic target? Curr Opin Nephrol Hypertens life expectancy. These patients often respond well to percutaneous renal artery angioplasty. If BP can be controlled to goal levels and kidney function remains stable in patients with ARAS, it may be argued that medical therapy with follow-up for disease progression is equally effective over periods of 3–5 years. Multiple prospective — Figure 289-1: Examples of micro-CT images from vessels defined by radiopaque casts injected into the renal vasculature. These illustrate the complex, dense cortical capillary network supplying the kidney cortex that can either proliferate or succumb to rarefaction under the influence of atherosclerosis and/or occlusive disease. Changes in blood supply are followed by tubulointerstitial fibrosis and loss of kidney function.
Figure 2¶
Caption: FIGURE 289-2 A. CT angiogram illustrating loss of circulation to the upper pole of the Activation of the renin-angiotensin system produced rapidly developing hypertension. B. lesion is often part of widespread atherosclerosis and sometimes is an extension of risk factors. and declining kidney function suffered mortality rates in excess of 50% over 6–12 months, hence the designation “malignant.” Postmor- of tem studies of such patients identified vascular lesions, designated “fibrinoid necrosis,” with breakdown of the vessel wall, deposition of eosinophilic material including fibrin, and a perivascular cellular — Figure 289-1 (Page 2151): Micro-CT images demonstrating microvascular changes in the renal vasculature. The images show vessels defined by radiopaque casts injected into the renal vasculature, illustrating the complex, dense cortical capillary network. The images depict the transition from microvascular (MV) proliferation in early atherosclerosis to MV rarefaction in chronic renal ischemia, leading to tubulointerstitial fibrosis and loss of kidney function.
Figure 3¶

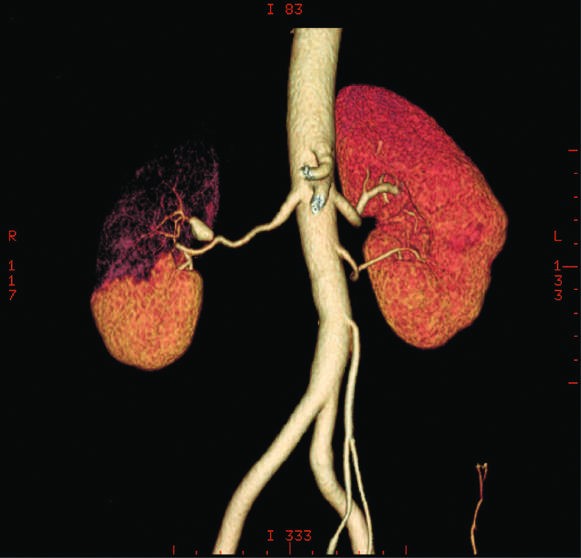
Caption: FIGURE 289-2 A. CT angiogram illustrating loss of circulation to the upper pole of the Activation of the renin-angiotensin system produced rapidly developing hypertension. B. lesion is often part of widespread atherosclerosis and sometimes is an extension of risk factors. and declining kidney function suffered mortality rates in excess of 50% over 6–12 months, hence the designation “malignant.” Postmor- of tem studies of such patients identified vascular lesions, designated “fibrinoid necrosis,” with breakdown of the vessel wall, deposition of eosinophilic material including fibrin, and a perivascular cellular — Figure 289-2 A: CT angiogram illustrating loss of circulation to the upper pole of the right kidney in a patient with fibromuscular disease and a renal artery aneurysm. Activation of the renin-angiotensin system produced rapidly developing hypertension.
Figure 4¶

Caption: Figure 289-2 B: Angiogram illustrating high-grade renal artery stenosis affecting the left kidney. This lesion is often part of widespread atherosclerosis and sometimes is an extension of aortic plaque. This lesion develops in older individuals with preexisting atherosclerotic risk factors.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.